The 2 vocal chords are the structures that make it possible to produce sound by modulating the voice.
The vocal cords can stop moving or partially (paresis) or completely (paralysis). Their lack of mobility may be due either to a mass that blocks (carcinomas) or block of arytenoid articulation between the ’ ’ and the cricoid cartilage (rare, for arthritic phenomena, traumatic or necrosis of cartilage) or, most frequent situation, for a non-nervous control of the vocal cords (ricorrenziale palsy).
Nerve pathways may be broken or the central nervous system or peripheral level. Your vocal chords are controlled by the inferior laryngeal nerves (or recurrent nerves) that detach from the tenth cranial nerve (vagus nerve) in the cervical, descend down to chest level (right subclavian artery and left surround ’ surround l l ’ aortic arch) and then go back into the neck (Why are also called recurrent nerves) going to innervate the larynx. Rarely, to the right, the inferior laryngeal nerve can go to innervate the larynx directly without descending into the thorax (recurrent nerve not applicable).
Given the complex Anatomy of recurrent nerves understands itself as many possible causes of paralysis ricorrenziale:
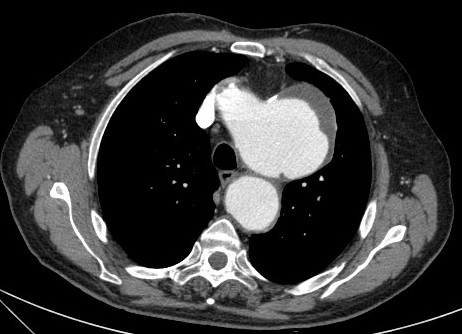
-peripheral causes: surgical lesions (thyroid surgery, cervical, chest strap, Esophageal perforation), thyroid tumors, Esophageal, tracheal tubes, lungs, trauma, toxic injury (quinine, lead), dell ’ subclavian artery aneurysms, aortic aneurysm, dell ’ left atrium dilation (Ortner's syndrome), Pericarditis, Mediastinal masses.
-Central causes: skull base surgery), Neoplasms,, ragged hole back syndrome, multiple sclerosis, Syringomyelia, encephalitis, stroke (Wallenberger syndrome), osteomyelitis.
Rarely you cannot identify a cause (idiopathic ricorrenziale palsy)
The vocal cord paralysis manifest with dysphonia, sometimes with dysphagia and rarely with Dyspnea.
The diagnosis is easy in transnasal flexible fiberoptic but the most important thing is to investigate the causes that may have caused the paralysis. And’ therefore often need to make a ’ neck ultrasonography and CT scan of the neck and chest with contrast.
To improve the dysphonia and dysphagia logopaedic therapy cycles may be used to help make the most healthy vocal cord so that satisfies that glottal closure guaranteeing a complete paretic in phonation.
There are also surgical procedures that have the ’ goal of “bringing” the two vocal cords so as to improve phonation and reduce ’ any dysphagia.








")
